
Plantar Fasciitis Pain Stops Here
Plantar fasciitis is a common cause of heel pain and mid-foot pain that can make standing and walking unbearable. Individuals suffering with the symptoms of plantar fasciitis often struggle to find a lasting treatment. There are several causes of plantar fasciitis. Symptoms may develop gradually over time or may be a response to injury. Foot pain can be very disruptive and limiting to regular activities. Fortunately, plantar fasciitis often responds positively to Rolfing Structural Integration and Integrative Bodywork techniques.
What Causes Plantar Fasciitis?
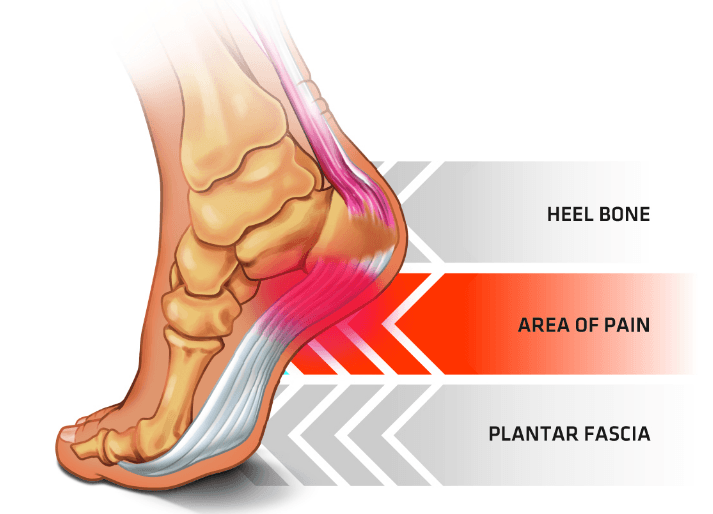
The plantar fascia is a layer of strong fibrous connective tissue located on the sole of the foot. Fasci-itis refers to an inflammatory reaction effecting this tissue. Pain may be felt at the heel or mid-foot area during palpation, standing, or in movement. The plantar fascia is a continuation of the posterior fascial line of the lower body. Past the heel, this layer becomes calf and then hamstring fascia before reaching the hips and low back. Due to the global connectivity of the body, plantar fasciitis can negatively impact the entire leg. Conversely, issues in the leg or even low back may produce pain similar to true plantar fasciitis.
Plantar fasciitis is caused by one of two phenomenon. In one situation, tension in the plantar fascia leads to formation of a heel spur. This abnormal boney protuberance creates irritation and is a source of pain. A far more common cause of plantar fasciitis is general muscular tightness and poor mobility.
Plantar Fasciitis Treatment:
Plantar fasciitis and heel pain generally respond rapidly to manual bodywork. When combined with Rolfing treatments and movement integration we have a truly powerful modality of care! Let us now look at a real example of how Rolfing techniques transformed a case of chronic plantar fasciitis.
Tammy’s story:
Tammy arrived for her first appointment with Dr. Eric at Rolfing Chattanooga with symptoms of chronic plantar fasciitis that was affecting both of her feet. She was previously diagnosis by her doctor and sent for physical therapy. Standing or walking for more than 30 minutes felt like an entire day of activity.Even light activity caused a severe increase in pain the next day. Tammy told me that her symptoms began three years ago after training for a 5k run. An inability to be on her feet made daily life challenging. Decreased activity contributed to weight gain. Physical therapy and chiropractic manipulations produced limited results. Tammy’s goal was to be able to walk without fear of next day pain and to participate in a kick boxing class.
“I had used inserts, sleep braces and actually had one foot in a cast and boot for 6-8 weeks. Nothing helped until Rolfing. Eric loosened up my legs and showed me that I was walking wrong. After 3 visit I can shop and enjoy life again.” Tammy, Soddy-Daisy, TN
I advised Tammy that she would need to come weekly for at least three sessions. We would use a combination of myofascial and Rolfing Structural Integration techniques. I told Tammy that even if she noticed major improvements after one session that it would be important to continue treatment to ensure that we are making a real change. Tammy agreed to three sessions and we began to work.
Knowing that Tammy’s pain began after training for a 5k run was a big clue that we were looking at a pattern of overuse and not a heel spur. Joint movement at the ankle and toes was reasonably good. Palpation of the plantar fascia revealed a few tender spots. Tammy added that her big toe also hurt at times. I moved my attention to her calves and the fascia of the lower leg.
Major movements of the foot originate from the lower leg. The leg is divided into four muscular compartments that are separated and organized by layers of fascia. The anterior and posterior compartments are responsible for flexing and pointing of the foot. Inside and outside compartments rotate and stabilize the foot.
Tammy’s muscles felt firm but lacked knots that are typically associated with an injury. When I moved her foot in and out of flexion it was hard to feel the corresponding action in the leg. This is the result of poorly differentiated fascial compartments. The sensation is of being bound up, like wearing a really tight sock.
A cross-section of the lower leg reveals the arrangement of four muscular compartments delineated by (blue) fascia. Each compartment contains multiple muscles. (Yellow) The tibia and fibula; (red) skin boundary. Plantar fasciitis is often associated with tightness of the posterior compartment.
We began work on Tammy’s calves. I wanted pointing and flexing of the foot to be clearly visible in the lower leg. I wanted to be able to feel the muscular action in my hands. Finally, it was key that Tammy feel the different movements and to know where they originated from in her body. As the layers of fascia separated the range and ease of motion increased. Each foot felt more connected to its leg. Furthermore, each leg felt more connected to the entirety of Tammy’s body.
I asked Tammy to stand and walk around. She moved delicately as if balancing on feet that were too small for her body. In truth she was not using her whole foot to walk. I asked her what was missing. After a bit more walking Tammy declared, “my toes!”

An active toe hinge is critical for proper walking mechanics. After heel strike weight is transferred to the ball and toes of the foot. This stretches the plantar fascia and allows for proper kinetic movement throughout the foot, leg, and back.
When walking we should make full use of the bottom of the foot. This means landing on the heel and transferring weight to the ball of the foot and finally to the toes. When the bottom of the foot is irritated by symptoms of plantar fasciitis it is natural to adopt a new style of walking that reduces pain by minimizing use of the foot. Over time this strategy effects organization and tone of the leg. There can be major disturbances along the entire kinetic chain. I asked Tammy to be active with her toes by pressing them into the ground when walking. We practiced walking forwards and backwards to get a better feel for the toe hinge in movement.
Proper Shoes:
Tammy returned after one week for a follow up appointment. She had been walking more and actively using her toes. She said there was less pain on most days except for one. I asked how that day was different. She said she was wearing flip-flops around the house. Now, I don’t have anything against flip-flops but they are not appropriate for everybody. Tammy is a perfect example of how footwear can lead to downfall. She needs to utilize her toes more when walking but wearing flip-flops causes the exact opposite to occur. Instead, toes flex down to hold the thong. Control is enforced from the foot to prioritize “keep this shoe on” over “walk appropriately.” I told her, “the flip-flops have to go, at least for now!”
Tammy was looking forward to a road trip which would include a visit to New York City and lots of walking. This would be a great opportunity to test the effectiveness of the bodywork. We spent the session freeing the fascia relating to Tammy’s toes. This work has a major influence on the entire leg up to the hips. I made sure Tammy would be sitting in a comfortable supported position during the car ride. I asked her to take breaks from sitting to walk when possible. I also asked her to keep her legs and feet active when in the car by writing the alphabet with her feet.
Walking Back to Health:
At her third session, Tammy reports that she had a great vacation and did not experience any pain after walking for six hours. This is a very encouraging result and it seems like Tammy is well on her way to meeting her treatment goals! It is important at this time that Tammy get back to living without the fear of painful plantar fasciitis. She has done a great job at being an active responsible participant in her recovery. She does not need any encouragement to stay active.
Tammy’s legs are moving so much better than a few weeks ago. The muscle compartments are well defined. Good walking mechanics require adaptability in the bones of the lower leg. The tibia and fibula function as shock absorbers during each heel strike. Impact force transfers into a fascial structure called the interosseous membrane. We work this aspect of the legs which also requires opening the lateral knee.
Tammy’s walk has taken on a whole new character. Using the entire surface of her foot engages every aspect of the leg. The plantar fascia is no longer bound in the calves or held up at the toes. The bones of the lower leg allow a better transfer of force through the knee to femur and hip. This will reduce the chance of Tammy experiencing future knee and back pain.
Plantar Fasciitis Treatment – Conclusions:
It is important to know that your body is always able to heal. If you have plantar fasciitis I want you to know that Rolfing Structural Integration and Integrative Bodywork are very powerful approaches to recovery. Combined with simple natural movements and easy self care it is very possible to achieve a rapid and lasting recovery.
Please leave a comment if this article sparks your interest in Rolfing Structural Integration or Integrative Bodywork. You can also send me a direct message or schedule a consultation. I look forward to your recovery and well-being!